
This is a page for member essays (not academic papers) and commentary on the state of teaching medical English, particularly within Asia. If readers wish to post an item, please send it through the contact us page and, after checking and possible editing, it will be posted. The current items are outlined below:
August, 2020:
- Covid-19 in Vietnam (a report)
- COVID-19 in Japan – What’s the situation?
- A Nurses’ Covid-19 Stories from Japan
1. Covid-19 in Vietnam

(courtesy of Minh Nguyen Thi Tuyet, Can Tho University)
Vietnam was successful in controlling the spread of Covid 19 in community for 99 days after the first wave of the pandemic. People seemed to return to their normal lives in spite of the government’s warnings of ‘the new normal’. Tourism companies launched attractive programs to appeal to domestic tourists with the hope of reviving the tourism industry. Tourists were eager to travel to their favorite places after days of high vigilance and Da Nang was probably one of their choices.
Suddenly, the first case of Covid 19 confirmed in a renal unit of Da Nang hospital in late July marked the beginning of the second wave of Covid 19 in this country. The number of new cases was on the rise in this hospital and spread to nearby communities and some neighboring regions. Thousands of travelers flying back to their homes made the airport and airlines serving Da Nang and several quarantine areas overloaded. Of course, such measures as isolating the hospital, visitors who had arrived at the hospital, tourists who returned from Da Nang, the city of Da Nang and social distance orders in Da Nang and other hotspots were carried out. Illegal immigrants were also traced and quarantined. Those who helped illegal immigration were fined. Regions adjacent to neighboring countries like China, Laos, Cambodia have been strictly supervised. All citizens, families, organizations and health authorities must be watchful and comply with Covid 19 prevention and control measures.
Despite the complex developments of the pandemic, the national high school graduation exam still took place as planned, except in Da Nang and Quang Nam. These two provinces would hold the exam 2 weeks later. Ultimately, this exam was safely and efficiently held.
The Covid 19 outbreak in Da Nang has been contained recently with all-out efforts. It could be said that the pandemic is within control in Vietnam. In Can Tho, my city, people have remained vigilant. Wearing masks is compulsory in public places and my school is not an exception. However, there have been some funny situations in my workplace.
To begin the new school year, there have been several meetings and conferences. All meeting members and conferees came to the events wearing masks but sat next to each other. All the masks disappeared at tea break. People chatted, ate, drank tea happily (including me) then most of them came back to the meeting hall without wearing masks. Of course, the speakers at the conference didn’t wear masks. It seems that people in my school wear masks to feel a sense self-prevention although they know that it is not really effective.
From the coming week, we have to teach face-to-face. Social distancing is impossible among students. What about mask wearing? We have to, but how long we can maintain this and whether it is effective are still questionable.
2. COVID-19 in Japan – What’s the situation?
COVID-19’s story in Japan has, so far, been a rather odd and unpredictable one. Early on in the pandemic, Japan was performing ‘so-so’ by international standards, but the mortality rate was of concern, this being the most aged population on earth. Thus, in May, national emergency measures were enacted. 90% of the country shut down. Even Japan’s ever-hustling workforce was asked to ‘stay home’. Schools of every stripe were closed (elementary, JHS, and HS from early March).
The interesting thing about these measures was that there was no legal compulsion behind them – one could not be arrested or fined for not observing them. This being Japan, it was expected that most people would comply for the simple betterment of society, with social pressure exceeding the legal kind (this is one reason that I enjoy living here – there has been virtually no infringement of personal right or privacy during the whole pandemic).
There wasn’t any massive, widespread testing – by design. Instead, efforts focused upon protecting the vulnerable, identifying clusters, and contact tracing. The role of the authorities has not been as liberal as the Swedish model but not nearly as strict as many other countries.
And it worked. At first. New cases dwindled to a low of 15 per day in late May as pretty much everyone in the country restrained themselves. It looked like we had achieved the same successes as Taiwan, Vietnam, and Thailand (relative to population). And as a result, quite naturally, the Emergency Measures were dropped. The economy was hurting badly – it was time to carefully move forward.
Most expected a subsequent rise in the number of new cases, especially since the drinkers and party people could now let their guard down a little. And after all, group drinking is a standard feature of Japanese society. Moreover, the government started to promote a domestic travel campaign in order to kick start the economy. But…
Well, you may have seen some frightening numbers in the news from Japan recently: for example there have been some days with over 1500 new cases in the past month, although those numbers seem to have levelled off and decreased recently. However, since the summer began, the vast majority of these new cases have been among young people, and the vast majority of those have been either asymptomatic or displaying only mild symptoms. While the raw numbers are up, the mortality rate has decreased significantly (echoing Western Europe in this regard).
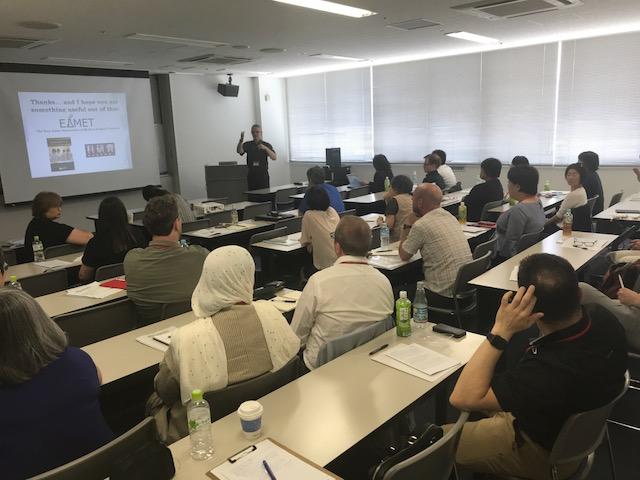
Most colleges and universities moved to online programs for the academic year beginning last April. (As you might have noticed, online classes have limited value – teachers cannot interact directly with students, spontaneity is decreased, and there is less sense of flow. Testing is very hard to conduct. And if lectures are recorded, many students admit to turning them on but not watching them).
At my own university, far away from the Covid-19 hub of Tokyo, we operated a hybrid scheme. The first month was all online, then, with several formalities and restrictions in place, we were able to teach face-to-face for the majority of the semester (teacher’s choice). However, a sudden spike in cases in Miyazaki Prefecture pushed us online again just as the semester was ending. As of September, kids are back at school and we expect to start the October university semester teaching face-to-face.
So, how does it look and feel on the street out here in Miyazaki? Mask wearing in any building is at about 99%. The protocols are clear and visible everywhere – the Japanese tend to be rather germaphobic even at normal times, so vigilance is quite high. Foreign travel is virtually impossible, but even travelling to other prefectures is widely frowned upon (and not allowed in many companies/institutions). Restaurants and bars are open but, of course, all kinds of public events and gatherings have been called off. Shopping and pleasure traffic is noticeably down in the core areas.
However, in many ways, a type of prevention fatigue has set in. People still follow the protocols but young people in particular are clearly beginning to think, ‘Is all this sacrifice and restraint really worth it?’ This sentiment has been echoed by the healthy aged too, who often have little left to look forward to if basic social pleasures are denied them.
There is no sense of fear anymore, more of long-suffering annoyance if anything, and the attitude seems to be that maintaining the current level of self-restraint should be sufficient – especially as so few cases currently seem to require any meaningful medical treatment, let alone result in death (in Miyazaki Prefecture, for example, there are currently 0 serious cases and there has been only 1 death). It seems almost impossible to eradicate the virus through policy or effort, as people in New Zealand and Vietnam know well.
This is a country that has dealt with several national crises in the recent past and, while cautious, this resilient quality has allowed the Japanese to gradually adapt to the ‘new normal’.
3. A Nurses’ Covid-19 Story from Japan

Many of our previous students are on the frontlines fighting COVID-19. Here is a story about one of mine:
I keep in touch with a handful of my old nursing and medical students. Most of our exchanges revolve around the predictable: our current activities, health, marriage and/or kids. Our jobs are rarely, if ever discussed. At least that was until COVID-19 entered the chat room.
One of my nursing students from Fukuoka texted me to say that she was being transferred into the infectious disease department – this was late in March of this year, just as Fukuoka Prefecture started seeing a sudden influx of COVID-19 cases.
A few weeks later she sent a follow-up text. Yes, she had regularly worked in ‘the ward’ and, perhaps unsurprisingly, she was exhausted. It wasn’t the length of the shifts – that hadn’t changed. Nor was it even the bulky protective wear. Rather, she said, it was constant gravity of the situation, the chronic sense of crisis and uncertainty, the perpetual sense that all the healthcare workers were playing with fire – under a magnifying glass.
And yet she added that while she came home after each shift with little more than enough energy to shower, change, and fall into bed, she had never felt so vital as a nurse, sensing that her work, of which so much previously had been drudgery and routine, now made an enormous difference in people’s lives. Now, her work MATTERED.
She wrote to me of one patient, an overweight man in his 30s who had contracted COVID-19 which, combined with his underlying comorbidities, was starting to take a grave toll on his body. Her team had just finished treating him during their rounds and were about to move on to the next room when she caught a glance of his face, glazed through the ventilator they had attached to him. There was a questioning, helpless, desperate glaze in his eyes – eyes fixed upon her own — which manifested itself a moment later as a tear. The man was terrified.
She stayed for a few moments after her team left the room, placing a gloved hand on his own and looked into his eyes, trying, she told me, to display compassion, strength, and confidence. She did not say a word. Staying those few extra seconds, and looking directly at his face, she told me, wasn’t much but it felt like the best she could do.
It was, in my opinion, the perfect thing to do.
At the height of Fukuoka’s surge, city workers and officials gathered in the adjacent parking lot to offer applause – a touching gesture of gratitude that had been echoed in many locations throughout the world. My former student was told that she could take a bow for twenty seconds, during which she could see and hear the applause of the crowd below. As her team lingered by the 4th floor window, she felt her own tear forming…
March 16, 2020: The COVID-19 Pandemic — What it says about Medical English Education and the Regional Cultures of East Asia
I’ve watched with interest, and some alarm, the worldwide spread of COVID-19 since the earliest outbreaks in Wuhan, PRC in January, 2020. Doubtless many readers have too. There is no reason for me to here repeat what a thousand media outlets are already saying so instead I would like to apply a perspective as it relates to both our profession and our region.
The pandemic seems to be winding down in China, with only a handful of new cases being reported each day, the majority of these now being imported from outside China. It appears that China has largely managed to get the virus under control. As a result, as the epicenter of the initial pandemic, there is much the rest of the world can learn from China, their crisis management, testing, and curative successes and failures can serve as lessons to others. But, of course, such information will largely come through English. The ability to write up and convey COVID-19 data, treatments, management, epidemiological reports in English now becomes paramount. This, friends, is why we do our jobs.
All of East Asia has a lot to offer the world in terms of its medical care, treatments and systems. Taiwan and Vietnam have (so far) maintained relative strong control over the numbers in both locales despite proximity to the epicenter, as have Thailand and Indonesia. Thailand was the first country to report a possible effective treatment (something similar to an ‘AIDS cocktail’). This needs to be heard, and further tested, by the rest of the world. South Korea has carried out the most comprehensive public testing of any country, even utilizing drive-thru check centers. The world can learn from this. Public action in Vietnam to trace and confine carriers and quarantine entire neighborhoods to limit the spread has been impressive. The ability to coordinate a carry out a quick, effective preventative response with public cooperation has been applauded by much of the world and should confound those who hold prejudices about the abilities of such countries to enact progressive policies. And again, the factors and features of these practices need to be disseminated to the rest of the world in English!
I feel (perhaps like many of you) that many in Western countries still harbour prejudices towards E. Asia. In fact, cases of xenophobic attacks of people who appeared to be E. Asian were widely reported during the early part of the crisis. Others questioned the abilities of East Asian medical skill and practices or the ability of the public and/or authorities to enact effective policy. And even when they did, many in Western media and social media decried this as authoritarian, draconian, or heavy-handed. But now, as the center of the pandemic has shifted to Europe, we see Western countries carrying out similar measures.
There are actually certain social/cultural features endemic to E. Asia which work in favor of defeating or limiting a pandemic like this, and even within the region it can vary between countries and cultures. Here are a handful that very few people are talking about but I think need to be considered
- The virus is less transmissible in hot, humid locales (this refers to affected surfaces; aerosol born spray from coughing or sneezing is still potent). This favours countries like Indonesia, Cambodia, Thailand, Myanmar, and the south of Vietnam.
- In North East Asia (plus Singapore, Malaysia) there is widespread, efficient, public transit used by millions. The quality is equal to, and often better, than found in the West. Unfortunately, these also serve as transmission containers and routes. In the less developed countries, people tend to travel on motorbikes or private cars more, limiting the spread. Less development also means that the average Cambodian, Indonesian, or Burmese is not jet-setting around the world but staying closer to their home as a matter of course. We might even say that COVID-19 is a rich man’s disease. Hence, the lower infection rate in such countries.
- Countries with less developed infrastructures may be more prone to bacterial epidemics (and some in the region have histories with this which may have helped in terms of enacting containment policies) but COVID-19 is a virus.
- While social distancing is easier to practice in places like Canada and Finland simply by force of nature, it must also be said that, despite the highly concentrated populace, most of E. Asia is not a kissing, hugging, handshaking culture. Nor, on the surface, does face touching seem to be as common as it is among Westerners and those from the Middle East. This also limits the spread. Exceptions to these are the Chinese habits of spitting (much, much less common in other parts of E. Asia) — which is slowly dying out as the populace becomes wealthier, better educated, and more sophisticated — and S. Korea and Japan’s widespread communal drinking cultures, which have been behind to the formation of some identified COVID-19 clusters (Thailand too). I can tell you that at the moment, the drinking culture of Japan is a rather forlorn one with most such parties being banned or cancelled.
Despite the social and economic impact COVID-19 is having (as well as its obvious health toll), all such events can serve as learning opportunities for the entire world. There is, and will be, much to learn from both the analysis and treatment of the virus itself and in terms of public health management. An event like this can help to shape cultures for the future. E. Asia has much of great value to contribute to the world in this regard, but it will have to be carried out in English.
And I hope that makes you feel a little more positive about your role as medical English educators in these troubled times.
(Addendum: One reader wrote to mention that another factor affecting the spread of the virus is a different underlying concept of human rights. She stated that in much of E. Asia there is likely to be greater social compliance when authorities require that restrictive protocols be carried out, whereas this is less likely in many Western cultures where people may see such authoritative measures as a violation of their human rights.
I agree, and would add that social trust between members of a society and those authorized to make or carry out decisions (not necessarily a blind trust in the government, but more a belief that adherence to established social systems benefits more people) is more prevalent in E. Asia than in the West.
Jan. 2020: The ‘Medical Humanities’ — Should healthcare English teachers adopt this ‘holistic’ approach?
The notion of English teachers as being primary agents in the practice of teaching the ‘Medical Humanities’ (MH) has been gaining traction worldwide in recent years. If I could sum up what is meant by the term, it would look something like this: The ‘English as a vehicle for teaching the medical humanities’ approach refers to the confluence of social, interpersonal, cultural communication skills, plus a holistic understanding of the patient-healthcare worker relationship in a manner that goes beyond the strata of purely clinical communication. It attempts to join the produce of the Humanities (Fine Arts, Languages, Sociology/Philosophy etc.) with the scientific/clinical perspective of healthcare workers. A number of assumptions and ideas have been included under the umbrella of the term the ‘medical humanities’ and, here, I’d like to list some of the positive, as well as problematic, notions I can see within the domain.
The valuable:
1. At the recently concluded EALTHY Conference in Spain, Dr. Jim Parle of Birmingham University (U.K.) claimed that clinicians should recognize that patients are not ‘objects’ or ‘cases’ but are actually experts in the field of themselves!
2. Above and beyond the traditional focus upon generating a diagnosis, clinicians should be aware that the greatest concern for patients is not just knowing what the diagnosis is but what this means for their lives, including management and follow-up — how will it affect them fully as a person? How will it impact their daily lives? How can it be managed and at what personal cost?
3. ‘Taking’ a history should be seen more as a collaborative process between patient and clinician and not merely as a series of Q-A as if it were an interview. History taking should be a matter of eliciting the patient’s story, allowing the patient to generate a narrative, rather than being a doctor-centered line of inquisition.
4.Gaining the patient’s trust to elicit personal/private/sensitive information, through implicit or direct request for consent, is a skill that doctors should learn to master. Using open-ended interpersonal skills, as opposed to closed question formats, should be encouraged. ‘Tell me more about that’ becomes (perhaps) the most common and helpful healthcare worker utterance.
5. The ICE formula (eliciting the patient’s Ideas, Concerns, and Expectations) should serve as the fundamental ‘template’ for history taking. More of the doctor’s time is spent listening rather than asking questions in such a scenario.
6. False empathy, such as the popular ‘I have a slight fever’ ‘Oh! I’m so sorry to hear that’ type of exchanges should be discouraged.
The questionable:
1. Often, the implicit assumption made by proponents of MH is that those of us with background in the humanities are more sensitive, aware, moral, and humane than those who come from STEM backgrounds. STEM people, the subtext seems to say, need our input to understand people’s feelings and to create more interpersonally effective communication and holistic care. As if STEM people are either insensitive or oblivious to these factors and thus require ‘our’ help. I, for one, do not buy this at all and I think it panders to outdated and negative stereotypes while allowing those of us from the humanities to pump our own chests.
2. While English teachers should be expected to understand how effective communication is constructed (especially in a foreign language), very few of us have the counselling or psychological backgrounds needed in order to feel comfortable about including such content in our teaching arsenal. We are not experts in sociology, philosophy, anthropology etc. and we should not assume to enter that territory with any authority. Let’s not overstep our bounds under the assumed banner of our ‘greater humanity’.
3. Concerns about the nomenclature (e.g. that ‘history taking’ is a presumptuous term and that ‘eliciting the patient’s story’ is preferable) seems to me to be window dressing of the virtue-signalling variety. The reality of the speech event or interaction is the same thing regardless as to how we label it.
4. Given the time limits and stressful workload that most doctors face, is it reasonable to believe that they should be behaving like counselors, spending a lot of time trying to suss out each patient’s ‘story’. Is it realistic? Doctors are not social workers.
5. In some respects, I don’t think MH crosses cultures particularly well. Even indirect attempts at prying into the ‘deeper’ personal aspects of a patient’s life will surely be viewed as intrusive and inappropriate by many Japanese (and other Asian) patients. Many, if not most, might want, prefer, and expect the standard Q&A routine. The doctor should stay in his/her territory and not assume other ‘roles’. This is extremely important within East Asian milieus.
6. I’ve asked several clinicians and medical students how they rank the following qualities among doctors: a) Communication skills b) Clinical knowledge c) Hands-on skills d) Humanitarian principles. ‘D’ almost always comes in last. If you’re not convinced, imagine that you are a patient facing a life-threatening operation. Which 2 are your priorities? Of course ‘D’ might be more of a concern if and when choosing a GP for long-term purposes but, again, this does not suit most Asian clinical milieus.
Other essays and reports:
2.English medical education in Myanmar- A report
3. Interviews with clinicians in SE Asia on the role and function of English for Medical Purposes
4. Medical English Teaching in Vietnam — A Report
5. Are EMP Teachers Ignoring the Horizontal Axis of Medical Discourse?
6. Medical English Spoken Discourse: Beyond Terminology
Questions from members to members can also be posted here. Please respond through the contact us page.
1.Positioning ourselves as EMP professionals- Michael Guest (EAMET Coordinator)
Having traveled to several countries in East Asia and meeting with several EMP teachers in the region, a common theme seems to have emerged:
EMP teachers are often misunderstood by administrators and clinical staff, treated as outsiders, as if their only value is their ability to speak English. This can lead to several negative effects. Administrators might feel that EMP teachers are not really academics and therefore dictate or enforce classroom and curricula policies and practices that they know little about, which can have an adverse effect on the students’ education. Or clinicians who are not really teachers may take it upon themselves to carry out the English teaching burden, when they are not qualified as language teachers.
Of course, we recognize that clinicians have a greater impact upon society, and that the promotion of English expertise among medical workers should exist mainly to allow for positive clinical outcomes, but we are less likely to achieve these outcomes if we are thought of or treated as mere ‘English speakers’. Sometimes, clinicians are better speakers of English than the local EMP teachers which can make them feel redundant or marginalized but we do have something unique to offer.
Here is what we offer (or, what we should be able to offer) as EMP professionals:
We don’t just ‘speak English’, we KNOW the language.
We know how to teach and manage a classroom. This was our training.
We know how to make suitable materials and develop comprehensive curricula and syllabi.
We understand how specialized English discourse works. No matter how fluent in English a clinician may be it is unlikely that he or she will have expertise in understanding the management of complex discourse models.
Let’s try to position ourselves as valuable, essential members of the medical humanities, as players within the healthcare community – and not just as ‘the campus English speaker’ who can teach daily conversation or translate documents. Let’s justify ourselves as professionals to clinicians and administrators so that our work and skills are valued and contribute to the advancement of medical communications
REPORTS and ESSAYS:
2. English Medical Education in Myanmar (Jan. 7-12, 2019) – a report

above: Yangon University Faculty of Medicine

-
- Myanmar represents a slightly unusual entry in terms of the use of medical English and its role in teaching and learning medicine. How so? Read on…
While in Myanmar in early January of this year, I visited with and interviewed four English speaking physicians, two fully devoted to their practice, two of whom are also actively involved in teaching at medical schools.
What readers should note first is that Myanmar is distinct from Thailand, Vietnam, Japan etc. in that it was colonized by England for a considerable period of time, during which English not only served as a de facto second language, but was also equal to a primary language for many educated/professional people, administrators, and educators.
While the legacy of colonial English remains, almost all Burmese currently claim that English skills countrywide have dropped considerably since independence, accompanied by an increased sense of national identity and local autonomy. These days, English is spoken quite competently by the educated/professional classes but not too widely or fluently elsewhere.
At universities, like most other countries in the region, the teaching language is the national language, Burmese. However, each doctor I talked to said that medical classes usually fluctuate (or code-switch) between English and Burmese largely because so much medical jargon and common academic phrases are more easily understood in English. One reason for this, perhaps greater than the legacy of British colonialism, is that medical textbooks and related study materials will almost certainly be written in English.

above: The magical Shwedagon Pagoda – Yangon’s hallmark site
Myanmar’s biggest handicap now is economic. The country cannot afford to attract or import foreign teachers who are trained in EMP/ESP, nor do they have the luxury of being able to train their own medical educators to teach using an EMP methodology. Basically, as is common in the region, medical instructors teach content (to some degree) in English – but the focus is upon conveying medical content, not upon developing specialist English skills per se.
Burmese doctors’ heavy workloads, particularly within the public sector, means that there is little time for furthering one’s English abilities within professional venues such as conferences or workshops. The chances to present or collaborate abroad are few because financing is difficult. Competition for funding to study or research abroad is fierce. As a result, upgrading English skills generally occurs only when foreign professionals visit Myanmar to carry out workshops.
While in Yangon, I briefly attended a small medical conference at which some foreign presenters were present, and the response from the local Burmese medical community in terms of attendance and participation was impressive. This was a rare opportunity for Burmese medical practitioners to share their research in English with peers from abroad.
Since high scores on English entrance exams are required to enter the better medical schools (such as Yangon University) it is typically children of the well-to-do, those who already have an international pedigree, who populate medical students at such institutions. The biggest problem however is the possibility of atrophy or even a decrease in English skills if they are unable to carry out any research or practice abroad and opportunities to learn/participate in English even in their own country are limited by the economic situation.
However none of this seems to decrease Burmese doctor’s eagerness to improve their English skills as they are extremely hospitable to those who might be willing to help.
3. Notes from interviews with non-native medical English speaking teachers, students, and doctors in SE Asia
While on research sabbatical in Thailand in late 2018 and early 2019, I derived a series of interview questions used to ask program teachers, clinicians, and coordinators about the role of EMP teaching at their own institutions.These interviews with medical English education program teachers, doctors, students, and coordinators elicited some compelling qualitative data. These are summarized below,
Prominent among the findings is the fact that very few medical institutions in the region operate or adhere to an explicit English for Medical Purposes (EMP) program. Busy clinicians are involved in English content sessions but do not serve as language teachers. Instructors who are trained specifically as language teachers are often called in or serve as volunteers from outside the university but lack clinical knowledge. Clinicians are not always confident with the quality of their own English but, more importantly, are often uncertain how to manage it as a class or lesson.
In practice, English often becomes combined with the native language in interactive sessions requiring a great degree of code switching by participants. This, however, is not a negative feature in a non-native English setting, particularly within the field of medicine in which specialist terms are often more readily and easily presented in English.
Further, my interviews revealed that the primary role of English is viewed as a source of research for production (online research, academic papers, conference presentations, collaborations) but financial or occupational constraints reduce opportunities to exploit this, leading to many English department coordinators and instructors to worry about atrophy or a decrease in the quality of their English production, which they fear may be passed on to their students.
Future applications
Regarding this research’s application to universities in the East Asian region in particular, I believe that the research uncovers or underscores the need for the university to hire or develop English teachers who understand medical discourse (EMP) and are trained in teaching specialist discourse.
General English teachers will surely struggle with creating and managing suitable clinical content while clinicians using English are often untrained in terms of classroom management or materials development. If English for Medical Purposes instructors are not hired, at least the clinicians teaching in English should undergo training in terms of English class management and materials/curricular development.
While clinicians can certainly create, understand, and carry out clinical case presentations on occasion they may lack the ability to maximize its potential as a participatory teaching/learning session.Specific training in the development of clinical English presentation skills among both students and resident clinicians would also serve as both a means of keeping up existing English skills and serve as a foundation for professional interactions such as international conference attendance, international research collaborations, and possible overseas research, study, or practice.
In none of the three countries I visited did foreign English-speaking patients constitute more than a miniscule 1 or 2% of all patients. Therefore, an educational focus upon doctor-patient discourses should be de-emphasized in favor of clinician-clinician medical speech events, of which clinical case presentations can serve as a core example, requiring the use of a combination of clinical, cognitive, and linguistic skills. The possible applications and utility of clinical case presentations as a core speech event are therefore more wide-ranging than any other speech event within the field of spoken medical English and they should thus occupy a central role in the teaching or application of medical English.
I wish to thank the staff and administration of Thammasat University, Faculty of Medicine, as well as those at Chiang Mai University, Yangon University (Myanmar), Hong Bang international University (Vietnam), Can Tho University (Vietnam), and Ho Chi Minh City Medical Center (Vietnam) for allowing me to carry out this research project on their premises with their approval and for supporting me with their kind assistance.
4. A Report on Medical English Education in Vietnam (June, 2018)

Hanoi Medical University
At the end of May, 2018 I took a 3-day research trip to Hanoi, Vietnam, where I met and discussed the medical English teaching environment with a number of local medical English teachers, as well as conducted interviews with doctors from various departments based at 4 different hospitals in the area.
One item of particular interest that I immediately noticed that is that many of us from outside the region tend to think that Communist/Socialist countries (or countries which otherwise have a heavily centralized bureaucracy) will have uniform systems in terms of their education practice and policy, this is far from the case in Vietnam, not to mention Japan, (and also, it appears, China). In fact, the policies and practices varied broadly from university to university.
The other quality that stood out for me was that most English teachers in Vietnamese medical schools had no background in medicine. While this in itself may not be unusual, in Vietnam teachers were required to go through some form of self-study to become familiar with the patterns and forms of medical English, as support via conferencing or specialist language training often involved having to go abroad, and they often did not have the funds to do so. Administrative support for such training is still in its early stages.
In some cases, Vietnamese clinical practitioners collaborated with the teachers but often the teachers were left to their own devices. This is an area in which organizations promoting the development of EMP, including an understanding of the scope and intrinsic features of medical discourse (both written and spoken), could prove to be very fruitful.
Many teachers also mentioned that some students gave up hope regarding any practical future use of English because they would be working within a fully Vietnamese workplace where English would not be needed, except perhaps for quick online searches and references.

Some of the other hopes, problems, and comments on the teaching environments of Vietnamese medical English teachers will likely parallel those in your own workplace/country, so I invite all EAMET members to read the full report. Below are some questions I asked, followed by a mix of typical responses:
- How many medical schools are there in Vietnam?
Most respondents said 12 or 13. These are the most prestigious institutions, although there are other institutions where students can study medicine but without the same pedigree or, it appears, with somewhat less rigorous training. Often, medical faculties are combined with pharmaceutical faculties.
- How many Vietnamese medical schools have English programs as a formal part of their medical education? What is the typical relationship between English classes and more clinical lessons in the curriculum?
In Vietnam, most, if not all, universities have set English programs and it is not an exception for medical schools. Each school will generally select their own teaching materials, curricula, program goals etc. In some cases, the English training component is incorporated or integrated into the Faculty of Medicine but, in many cases, the English teachers are considered to be generalists, outside the medical faculty. Some teachers mentioned that they felt isolated from, or were looked down upon, by medical practitioners and failed to be recognized or treated as academics.
- Do most medical schools in Vietnam include EMP as a formal part of their English education? How about your own?
Most schools appear to host both EGP (English for General Purposes) and EMP classes, with more classes being allotted to the former, particularly in the lower grades, often at a 2-to1 or 3-to-1 ratio. Most teachers mentioned that their class size is very large (often 50-80 students in each class). This means that discourse features of medical English, particularly speech, cannot easily be taught or practiced. Thus, there is an emphasis instead upon teaching terminology, particularly anatomical terms and disease names. This is often supplemented with other materials so that students can self-study.
- How is English education usually included in the overall medical school curriculum in Vietnam? How about at your own institution?
English is mandatory during the first and second year in most schools but, in one case, I was told that it is mandatory for only one year. Within that framework, the amount of time given for English study also fluctuates.
After the first two years are finished, it is often only within special selected (or elective) courses or interest groups (clubs) that students can advance their English skills. However, many textbooks are written in English as is almost all research so students also get exposure to the language (passively) this way.
- Are there any organizations promoting, supporting or furthering the training of EMP teaching in Vietnam? How about ESP?
No teachers I corresponded with or interviewed knew of EMP organizations in Vietnam. However, ESP is gaining a foothold, with seminars, a first national conference, and training programs increasing. Interestingly, there is top-down support from some national organizations in terms of funding to help teachers get training abroad (particularly Taiwan, Singapore, and Hong Kong). Not surprisingly, it is generally the very top universities that receive such funding.
- Does your own institution support or endorse EMP teaching explicitly? If so, in what way?
Most schools have no explicit EMP teacher training or EMP-oriented curricula or explicit teaching policy. In fact, a few respondents stated that the time allotted for EMP has been reduced. Most universities appear to see the development of syllabus and the materials for EMP as a product of teacher collaboration with doctors in rewriting the existing syllabus. However, a few teachers remarked that the widespread view of medical English is merely general English topped with a sprinkling of terminology.
It was also mentioned that a small percentage (5%) of teachers go abroad for specific training.
- What balance do you think exists between general vs. EMP teaching in medical school English classes in Vietnam? How about in your own classes?
For general English, most help students develop all four skills, with an emphasis on reading. About half of the teachers I interviewed used medical English textbooks, which required some collaboration with clinicians – it was said that it is difficult for English teachers to follow a medical English textbook as the basis of a course and thus was used more as a supplement.
Further, rather than discourse, many EMP classes focused upon teaching prefixes and suffixes or terminology. In short, general-medical content was integrated at about a 50-50 rate. Only one teacher mentioned a focus upon productive tasks or the development of medical discourse skills.
- What would you consider to be the most important teaching features or goals of an EMP class?
The most significant goal of EMP classes is to help students become more aware of the importance of English in their future career so that they can use English as a tool to explore the world of medicine or to simply increase medical knowledge (through reading research). For some, practical applications of EMP included a focus on developing presentation skills or discussion of topics related to hospital practice (this was limited to small, upper-level classes).
Many teachers cited listening and pronunciation as particular weaknesses. In the case of pronunciation, this can be particularly problematic as many medical terms have no cognate in Vietnamese and thus tend to morph into Vietnamese phonology.
- Outside of specific university English classes, how do Vietnamese medical students develop their medical English skills?
Many take part in English clubs. Keen students will also take extra classes (for credit) with doctors who are proficient at English. Some advanced students also volunteer to work with visiting doctors from abroad who come to the university. Post-grad students often must summarize their studies/research in English as a part of their graduation requirements.
- How do English teachers at medical schools in Vietnam get EMP training, if at all?
There is almost no training for English teachers in EMP. Most teachers have to self learn and there is little support from program directors and/or administrators. A few teachers expressed hopes for greater hands-on teaching in English within the affiliated hospital (with English-proficient clinicians) and improved cooperation with lecturers both inside and outside of English departments. One teacher called for clearer needs analyses to be conducted before designing EMP courses, keeping in mind that these should always be tied to practice.

The author’s general comments:
First, a big thank you to the teachers of Hanoi Medical University for helping me to coordinate my visit and for their helpful insights and care in arrangements. Also, thanks to two other teachers from Haiphong, whom I count as good friends. All the food you introduced me to was wonderful and, along with the gregarious personalities of the teachers I met, form my sharpest memories of Vietnam.
Vietnamese medical students and clinicians have a good reputation for their English skills when training or practicing abroad but I was surprised to hear that many local medical English teachers lamented their more average students’ lack of interest and/or proficiency in English – noting that it was often difficult to get students to concentrate in classes or to take them seriously.
I think one way to address this would be for many administrators to adopt more established and integrated EMP programs from the first year of university study. This means establishing more chances for training in specialized discourses for Vietnamese English teachers which would give them the confidence to venture outside the areas of suffix/prefix and terminology teaching. I believe that medical English teachers have to promote their skills within the university, to be viewed not merely as proficient English users, but more as specialists who understand, and can teach, how medical discourse works, both written and spoken, both in academia and in the workplace. In short, teachers should try to establish their academic niche at their universities in a manner that forces clinicians and administrators to fully understand their value in medical education. We don’t want to be seen only as standard classroom teachers who happen to be good at English.

The English teachers at Hanoi Medical University with the author
Collaboration between Vietnamese medical English teachers and those from other countries could help to realize this. If readers from outside Vietnam would like to establish contact or collaborations with Vietnamese medical English teachers, please feel free to send a comment to EAMET at http://www.med.miyazaki-u.ac.jp/home/eamet/contact/
Finally, if any Vietnamese teachers wish to add their voice or correct anything I have written above, I welcome their responses via the same link.
Michael Guest, June, 2018
5. Are EMP Teachers Ignoring the Horizontal Axis of Medical Discourse?
Michael Guest, University of Miyazaki (Japan)
Have medical English teachers largely neglected horizontal communication in favour of the vertical? What I am referring to here is doctor-to-doctor (or health professional-health professional) discourse (representing the horizontal axis), as opposed to doctor/health professional – to – patient discourse (representing the vertical axis). From what I have seen in textbooks and heard in presentations, observations, and discussions with medical English teachers, particularly in Asia, it seems that the great weight of teaching has fallen upon the vertical.
Perhaps this is because many medical English teachers (whether local or so-called ‘native English’ speakers) come from backgrounds outside of healthcare fields and, as such, their view of medical discourse is often coloured by the patient’s perspective – having only been patients themselves.
As a result, our teaching may tend to emphasize doctor-patient discourse, generally focusing upon history taking, a staple of most medical English curricula. History taking is, of course, an essential clinical skill, one that has washback value extending into the learner’s first language and culture. It should be a part of any EMP curricula. However, we might want to consider the actual odds of our learners treating patients who don’t speak the lingua franca of the hospital/country. Unless one works in an accredited international hospital or an area noted for medical tourism the chances of such doctor-patient encounters will likely be low.

Medical discourse has both vertical and horizontal dimensions
For example, in my own institution (in Japan) most requests for upgrading in English skills from clinicians arises from their wishes or concerns about applying these skills on the horizontal axis of discourse. As very few medical tourists or non-Japanese speaking patients visit our hospital, greater value for our clinicians is found on the peer-to-peer horizontal axis – the need for professional development or to become active participants in the medical discourse community. This is also true when training health professionals before they go abroad for research or practice.
The most obvious of these horizontal discourses are specialized peer-peer functions such as giving conference presentations or posters, as well as academic paper writing – and, indeed, some EMP teachers do try to practice these skills with their learners. But also, due to the increasing frequency with which healthcare professionals move to new international locations for research or practice, the ability to use English as a working language (whether as host or as guest) has become a vital skill.
One of the functions required in such cases is the ability to make a clinical case presentation. These can be more formalized ‘conference-style’ presentations given within a hospital department, peer-to-peer, or they can be the intense real-time conveyance of clinical data between two professionals during working hours.
Case presentations, like history taking, demand the use of critical thinking skills, the ability to organize data, the ability to grasp and express pertinence, and to separate such data from more peripheral items – in short, the management of specialized discourse. These skills too, when practiced in English, can have a washback effect on the learner’s first language or home working culture.
Horizontal English discourse skills can have an effect on the learner’s L1
What this means is not merely that EMP teachers should include case presentation skills in their syllabi, but that teachers should pay attention to how medical professionals actually communicate with each other in English-language settings. This would include having knowledge of which speech events occur most, among which types of clinicians, and to what ends and purposes. How are these events typically opened, managed, and closed?
Of course, in one’s home institution, these interactions will likely be conducted in the national language. But, for the sake of health professionals who will be going abroad or for those who will partake in international collaborations in the future, an ability to utilize the English of the workplace or the English of the internationalized professional will hold great benefits.
And even for those who do not plan to further their skills in an international setting, the increased awareness of clinical content, speech events, and interpersonal skills learned in English can carry over – or, again, washback – into one’s first language.
This horizontal axis of discourse deserves more exploration from EMP teachers.
6. Medical English Spoken Discourse: Beyond Terminology
Michael Guest, University of Miyazaki, Japan
Recently at our university, we conducted individual interviews with all our 4th year students currently participating in our elective EMP course. Two of our set questions for them were ‘What are you currently doing to improve your English speaking skills?’ and ‘What do you think you need to focus on most to improve your medical English skills?’ While some of our students are returnees from abroad and thus speak English with some proficiency, there are several who still struggle with real-time speech (both in general and medical contexts).
However, the answer to these two questions was invariably, ‘I have to learn more medical terminology.’ In some cases, this response was even further reduced to, ‘I have to learn more names of diseases.’ As a result, several students explained that their self-training consisted of noting new or unknown terminology in medical textbooks.
There is a tendency for students and the general public alike to think of medical English as basically consisting of general English + specialist terms. And, in my experience dealing with other ESP/EMP teachers, this belief often extends to instructors too. But is this notion accurate? Or even beneficial to learners?
The problems of teaching terminology
One problem that I have with an inordinate focus upon terminology is that it largely leads to learners memorizing single items from a list, rather than internalizing larger units of meaning through the practice of meaningful discourse. Moreover, prioritization easily becomes obscured as learners try to recall one-to-one matches based on the list. The almost endless parade of such terms can also become a hindrance.
There are several other problems. In many cases, the English term equals the local term anyway – with the latter often just transliterations of the English (or Latin/Greek) term. More pertinent as a criticism, perhaps, is the likelihood that learners will retain these items only instrumentally — until a test is given.
In fact, several young doctors I’ve interviewed told me that they really absorbed the specialist terms only when they actually entered the specialist department and were used as a part of daily discourse (in my doctors’ workplace, English terms are regularly sprinkled among Japanese discourse such that they have become de facto Japanese terms). While they had superficially ‘learned’ many of these in their early years as a medical student they had forgotten them until they were needed in practice (necessity being the mother of internalization?).
There is also a widely expressed viewpoint that terminology is ‘hard’ and thus requires specific attention from EMP teachers. First, terminology is not at all ‘hard’. Such items are usually nouns (thus are very distinct parts of speech) and have clear meaning ranges and very specific referents in other languages. They are rarely vague, semantically or pragmatically, and do not depend upon context for interpretation. They may be long and challenge one’s pronunciation skills, but as lexical items, they are hardly ‘difficult’. A teacher isn’t even required – any competent dictionary will readily provide concise translations.
Terminology is not equal to ‘professional discourse’
The real difficulties in fact lie elsewhere. For example, all the Japanese doctors in my own institution are proficient in using specialist English terminology, but many, even senior practitioners will say things such as, ‘the patient is cancer’ (Japanese particles of attribution do not match the English ‘be’ and ‘have’ verbs very closely). ‘Hand’ and ‘hands’ may be confused (the language also lacks explicit plural forms). They might confuse ‘the patient has had it for X’ (current duration) with ‘the patient had it for X’ (which assumes that the condition is finished). The greater problem, it seems, is with the horizontal use of language as discourse (and by this, I don’t simply mean ‘grammar’), and not with the vertical dimension of single-item lexical semantics.
The undue focus on terminology, however, also has the much more insidious uptake of perverting an understanding of what specialist discourse is. Medical discourse simply isn’t a plateful of General English topped with a sprinkling of specialized terms. We can see this clearly if we use academic essay writing as an example.
As you know, writing an academic paper involves structuring the paper in a certain way, often marked by specific sections in a set order, plus the use of certain set phrases and strategies. A scientific ‘narrative’ is employed to connect introduction to methods to results/finding to discussions to conclusions. Failures to use this narrative form might not only mean that readers become confused regarding the flow and cohesion/coherence of the paper but also that their paper will not be accepted for publication. The use of specialist terminology therein is only a minor consideration.
Spoken Medical English and Formulaic Academic Phrases
This focus upon maintaining a narrative carries over to medical spoken discourse. Almost all medical staff will have a grasp of the English terminology but many may struggle to use an appropriate English narrative framework (see the sections on this site regarding clinical case presentations). Even more obvious is simply sounding like an academic, a highly-educated professional. Note the following two examples:
- The patient has been coughing for a long time.
- The patient suffers from a persistent cough.
There is no specialist terminology involved here but I think we’d all agree that the second example is far more professional in tenor. This indicates not only how a doctor might actually convey data to another doctor, but also displays the type of formulaic academic phrases that mark conference presentations, academic papers, and general professional discourse. Such formulaic phrases (e.g., the oft-used combination of suffers+from+persistent X) mark an intermediary step between general English and specialist terminology.
These then, rather than lists of terms, with their connection to interactive discourse, and usage rather than meaning, are of a higher learning priority than terminology. Moreover, these are items that non-medical specialist teachers can/should have both knowledge of and an ability to teach. These are the building blocks, the workhorses, of professional discourse and should be treated as such.
As for those specialist terms, for the most part, we should leave them up to the students and the dictionaries. They’ll learn them when they need them.